I’ve spent the last week discussing the hypothetical case of a young patient with a stab to the abdomen. I worked through some of the thought processes regarding physical exam, imaging, and choices for management. Fortuitously, it would seem, The Journal of Trauma published an algorithm on this very topic from the Western Trauma Association (WTA).
The WTA Algorithm Committee reviewed existing data to start the process of developing this algorithm. As could be expected, very little high quality data was available. So the final algorithm is a synthesis of existing lesser quality studies, expert opinion from the committee members, and commentary from the membership.
Here are some of the highlights:
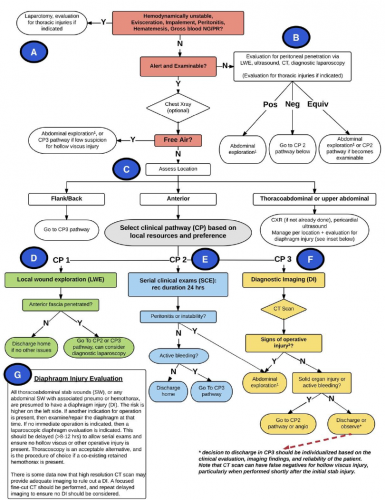
- Unstable patients go straight to the operating room (A)
- Patients who cannot be examined (unconscious, head injured, intoxicated) should be evaluated for peritoneal penetration with local wound exploration, ultrasound, CT, or laparoscopy. If positive or equivocal, proceed to exploration. (B)
- Patients who can be examined should be managed by location of the stab. Flank injuries are lower risk and should be scanned. Anterior stabs can be evaluated using observation, local would exploration, or CT scan,
- Positive results generally proceed to laparotomy. The algorithm states that laparaoscopy “may be performed in select stable patients by a highly skilled surgeon experienced in minimally invasive surgical techniques.”
As with any algorithm or practice guideline, nothing is etched in stone. These tools are good for about 90% of the clinical situations you will encounter. If you end up off the beaten path, you will need to use your best judgment to provide best treatment for your patient. Just remember to document your rationale, because you may very well have to justify it to your peers.
Click the diagram below to see a full size version.
 Reference: Evaluation and management of abdominal stab wounds:
Reference: Evaluation and management of abdominal stab wounds:
A Western Trauma Association critical decisions algorithm. J Trauma 85(5):1007-1015, 2018.
