Trauma professionals who don’t routinely take care of burns tend to radically overestimate the size of burns. This can create significant problems for the patient, because the formula used to determine fluid rates and total crystalloid given are based on burn size.
Don’t flood your patient! Watch this 5 minute video instead.
Last year, a lot of the papers presented at EAST were a bit ho-hum. But I’ve been reviewing the abstracts for the upcoming January 2016 meeting, and there’s a lot of good stuff! Although you do need to take this with a grain of salt, because sometimes the paper does not live up to the hype of the abstract. But many of the abstracts look so good, that I’m going to dedicate both December and January Trauma MedEd newsletters to reviewing them.
There are lots of intriguing ideas coming! Here are a few that I will be writing about:
Suction evacuation of hemothorax
(F)utility of CPR in hemorrhagic shock
(F)utility of blood administration in the helicopter
EMS scene time and mortality
Does Mucomyst (acetylcysteine) predispose to pneumonia?
Distracted driving prevention
How long is DVT a potential risk in TBI?
Plus I’ll pick apart a number of really crappy abstracts
And more…!
Anyone on the subscriber list as of midnight (CST) Sunday night will receive it later that night Everybody else will have to wait for me to release it here on the blog late next week. So sign up for early delivery now by clicking here!
This 11 minute video shows you how to insert an IV like a professional, with or without ultrasound. Two experts show you their best technique.
The video was broadcast during Trauma Education: The Next Generation 2015 and features Michael Zwank MD and Chris Norman RN from the Regions Hospital ED and department of Emergency Medicine.
Focused abdominal sonography for trauma (FAST) has been around in one form or another for about 40 years. Sonographic examination of the abdomen was used in Europe in the 1970s, while the US was using diagnostic peritoneal lavage (DPL). FAST finally moved to the US in the 1990s and continues to this day. It has also been incorporated in the Advanced Trauma Life Support Course sponsored by the American College of Surgeons.
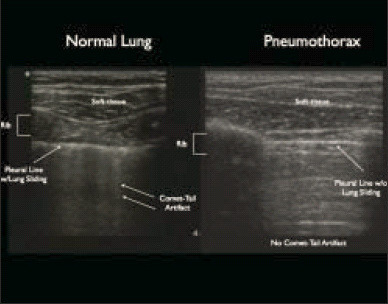
About 10 years ago, emergency physicians began using sonography to evaluate the thorax as well. The technique was primarily used to detect air (and possibly fluid) in the pleural space. Sensitivity and specificity have increased nicely over the years as the technology and our experience has improved.
Most trauma centers incorporate FAST into their trauma activations. Although it was initially vetted using blunt trauma patients, it can be and is used for evaluation in penetrating trauma. But relatively few centers expanded it to eFAST to evaluate the chest. Should they?
Bottom line: Definitely! Extended FAST adds about a minute to the overall exam and may provide information before the chest x-ray is obtained. It may also show pathology that the typical trauma chest x-ray cannot due to patient body habitus and supine positioning. I recommend that the eFAST be the standard of care in trauma activations if you have an ultrasound machine. Important! But be sure to have a way to record and perform quality reviews of the information obtained.