Here’s an interesting note out of the University of Pittsburgh. They are preparing to engage in a study to look at the role of hypothermic arrest as a way to salvage trauma patients who are bleeding to death. Sometimes we encounter catastrophic injuries that are exceeding difficult to stop the bleeding. Some vascular injuries within the abdomen come to mind, particularly retrohepatic vena cava injuries.
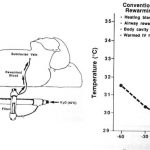
So what would happen if you rapidly reinfused the patient with cold preservative instead of more blood? The idea is to stop the heart and induce profound hypothermia that would essentially put the brain and other key organs into suspended animation. This might provide a period of time to do the needed repairs, but not worry about the imminent danger of brain death.
Sam Tisherman, the principal investigator, terms this scenario EPR or “emergency preservation and resuscitation” instead of CPR. The desired temperature after cardiac arrest is 50 degrees F, or 10 degrees centigrade. Animal trials have shown promise.
Bottom line: It will be interesting to see how this goes. We’ve tried hypothermia for heart attacks, head injury, and a number of other clinical problems. Unfortunately after initial enthusiasm, they’ve generally not lived up to their billing. It seems counterintuitive to use a maneuver guaranteed to produce coagulopathy to save somebody who is bleeding. But sometimes this type of bold thinking results in life-saving breakthroughs.