Hypothermia is the bane of major trauma resuscitation, causing mortality to skyrocket. A number of rewarming techniques have been developed over the years. These are classified as passive (the patient generates their own heat) or active (we deliver calories to them), and noninvasive vs invasive. Rewarming speed increases as we move from passive to active and from noninvasive to invasive.
Continuous arteriovenous rewarming (CAVR) is one of the invasive techniques used today. Its use in humans was first reported 20 years ago this month. Larry Gentilello at Harborview in Seattle had experimented with this technique in animals, and reported one case of use in a human who had crashed his car into icy water. After a 20 minute extrication, the patient was pulseless with fixed and dilated pupils, but he regained pulse and blood pressure at the hospital.
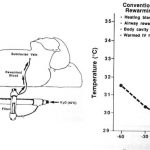
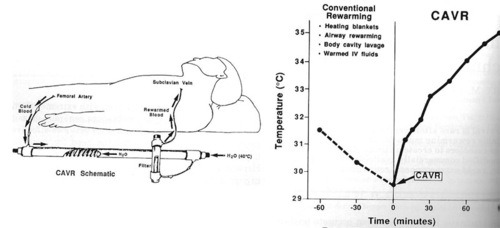
The initial core temperature was 31.5C. Peritoneal, bladder and gastric lavage were carried out for warming, as was delivery of warm inspired gas via the ventilator. However, after an hour the temperature had dropped to 29.5C. CAVR was initiated as a last-ditch effort using a jerry-rigged Rapid Fluid Warmer from Level 1 Technologies. The core temperature was raised to 35C after 85 minutes.
The patient did have typical complications (ARDS, acute renal failure), but survived with recovery of his renal and pulmonary function, and a normal neurologic exam. At the time, the authors were unsure whether the complications were due to the near-drowning or the rapid rewarming.
Reference: Continuous arteriovenous rewarming: report of a new technique for treating hypothermia. J Trauma 31(8):1151-1154, 1991.
Related posts: