They are the bane of trauma professionals, the anticoagulants that cannot be easily or cheaply reversed. Yes, I’m talking about the direct thrombin inhibitors and the Factor Xa inhibitors. They were originally called NOACs, or novel oral anticoagulants since they were newer than the old standard, warfarin. But they’ve also been listed as DOACs (direct) or TSOACS (target-specific, just rolls off the tongue doesn’t it?).
Here’s a nice table I put together recently showing the all the common oral agents available. Click the image for a full-size, more readable image.
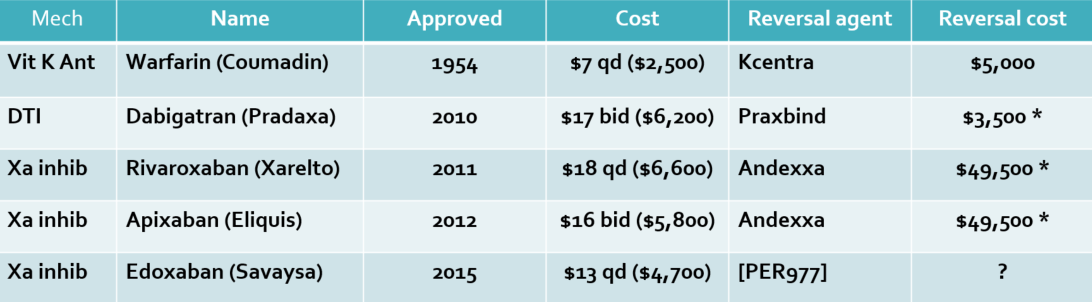
Dabigatran was the first of the newer oral agents, and it is the only direct thrombin inhibitor in the group. The rest are Factor Xa inhibitors. This is easy to remember if you look at their generic name. Each will contain “xaban.” Get it? Xa ban.
The daily cost of warfarin is about $7, while the daily cost of the others is around $16 per day. However, that does not take into account the cost of blood work to monitor INR in those taking warfarin, so it’s cost will be higher.
What I found most interesting was the cost of the reversal agents, if any. For warfarin it’s either a hit of 4-factor prothrombin complex concentrate or many bags of plasma. Praxbind for the DTI dabigatran appears to be a bargain! But look at the agent for the Xa inhibitors, Andexxa! Almost $50K per pop!
And what about the asterisk, you ask? That means that there is no literature available that shows that these expensive drugs are clinically effective! But they seem like they should work. Hmm.
Anyway, back to the nomenclature. NOACs or DOACs? Opinion is moving away from NOAC because it can be misinterpreted as “no anticoagulants.” The International Society on Thrombosis and Haemostasis polled their members, and the consensus opinion was that DOAC should be adopted for common use. They add that the specific mechanism of action (direct thrombin vs Xa inhibitor) should be specified in addition to the DOAC acronym when clinically relevant.
Bottom line: DOAC wins! So hopefully we can all converge on using one common term for this group of drugs. Yet I still shudder when I have a head injured patient that tells me they are taking any of them!
Reference: Recommendation on the nomenclature for oral anticoagulants: communication from the SSC of the ISTH. J Thrombosis Haemostasis 13(6):1154-1156, 2015.
