You are in the middle of a fast-paced trauma activation. The patient is awake, and mostly cooperative. The x-ray plate is under the patient and everyone stands back as the tech gets ready to fire the x-ray machine. At that very moment, your patient reaches up and places his hand on his chest. Or one of the nurses reaches over to check an IV site.
The x-ray tech swears, and offers to re-shoot the image. What do you do? Is it really ruined? They have an extra plate in hand and are ready to slide it under the patient bed.
The decision tree on this one is very simple. There are two factors in play: what do you need to see, and how hard is it to see? The natural reaction is to discard the original image and immediately get a new one. It’s so easy! But take a look at this example of a “ruined” chest xray.
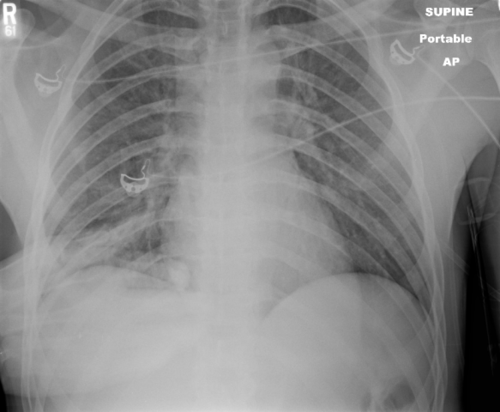
Bottom line: You are looking for 2 main things on the chest x-ray: big air and big blood. Only those will change your management in the trauma bay. And they are very easy to see, even if the image is cut off and off center. Couple that with the fact that an arm overlying the image does not add a lot of “noise” to the image. So look at the processed image first. 99% of the time, you can see what you need, and will almost never have to repeat. [Hint: the same holds true for the pelvic x-ray, too. You are mainly looking for significant bony displacements, which are also easy to see.]
Related posts:
- How much radiation is your trauma team exposed to?
- Repeating x-rays for patient positioning
- Repeat imaging after patient transfer
