Here’s some background info to go with the xray presented Wednesday:
- Thin
- Athlete
- Epigastric trauma
Put these three together and you get a patient engaged in significant physical activity who was struck in the abdomen. If no pads are involved in the sport, the patient has little padding of their own.
This is a setup for pancreatic or duodenal trauma. This patient presented after being struck in the epigastrium by an elbow during a soccer game. It hurt, but wasn’t bad enough to stop playing. The following day, she was a little sore but felt bloated and started throwing up after breakfast.
In the ED, a CT was obtained. Here is a coronal view showing the distended stomach:

Axial views showed obstruction in the proximal 3rd portion of the duodenum, right over the spine:
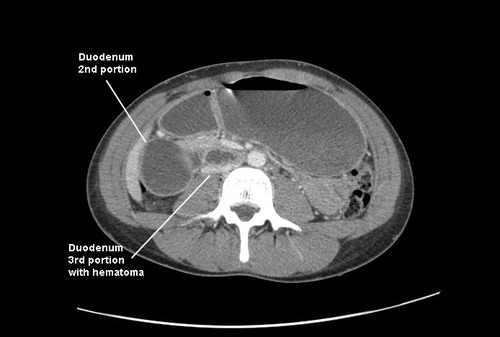
An (unnecessary) contrast study was performed, which confirmed the pathology. Note the tapering and corkscrew appearance of the duodenal folds.

Final diagnosis: duodenal hematoma. This is a crushing injury from compression of the anterior abdominal wall against the spine. The third portion of the duodenum lies over the spine, as does the pancreas, so both are likely to be injured. The latter organ appeared normal on the CT.
Management of blunt duodenal hematoma is simple: wait on it. These will generally resolve quickly over the course of a few days. NG decompression is mandatory, since nothing will pass the obstructed area (saliva, gastic juice, and pancreatic effluent, which add up to 2L+ of fluid per day). In rare cases, parenteral nutrition may be needed if resolution time is approaching the one week mark or in smaller children. A surgical approach with drainage of the hematoma has a low but significant morbidity compared to just waiting. Athletes may return to play soon after recovery.
