As described last Friday, this patient was found at home bloodied, obtunded, with his hand amputated. He was taken to the hospital (with the hand properly dressed, in a bag), then went to OR for reimplantation. The exact mechanism (assault vs self-mutilation) was not known at the time.
What happened to the patient? Inspection of the scene revealed no forced entry and no evidence of an intruder in all of the blood at the scene. It appeared to be self-inflicted. The hand surgeon determined that the hand could not be reattached. Postoperatively, the patient did not wake up appropriately. He was taken to CT scan and this image was obtained:
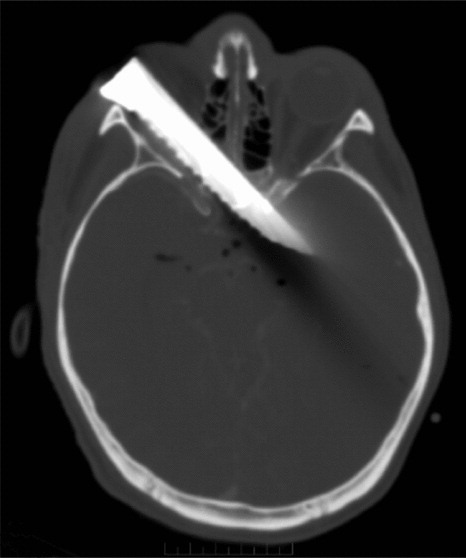
This explains the small laceration beneath the right eye. The neurosurgeon deemed the injury nonsurvivable and the patient rapidly progressed to brain death.
Was prehospital care appropriate? Absolutely! They stopped the bleeding, packaged the hand nicely for an attempt at reimplantation, and transported to the hospital quickly. By the way, physicians are usually involved in prehospital care in Europe, where this event occurred.
Is it likely the hand can be reattached? No. Although clean amputations have the best chance, this was likely a ragged wound because a table knife was used to saw off the hand. This takes a lot of force and effort and usually results in severe damage to the severed ends.
What other diagnostic tests should be performed, and when? The patient had two problems: a hand injury with easily controlled bleeding, and a brain injury (remember, the initial GCS was 11). A full evaluation should have occurred before transport to the OR, and this would have prompted an early CT scan of the head. Whether this would have changed the outcome can’t be determined.
Bottom line: this is another example of the “dang!” factor at work. Everybody sees this bloody patient with a mangled, severed hand and focuses on it. The rest of the ABC(D)s go out the window, and the patient is rapidly taken to OR to save the hand. But the knife used to sever the hand is hidden in his brain, and the team is unaware until attention returns to the mental status postop. Don’t let this happen to you!
Related posts:
Reference: An unexpected intracranial blade. Prehospital Emergency Care, online ahead of print, September 2012.
