Time for the answer! There were lots of well thought out guesses, and a few correct answers.
Here’s the story. This is a young male who presented in the trauma room with a small penetrating injury on the lateral aspect of his right arm, and another one just medial to the top of the scapula. If you look at first image last Wednesday, you can see an obvious humeral fracture, a not so obvious lack of lung markings, and a few tiny metallic foreign bodies (bullet fragments picked up by Canuck ER MD, injuries surmised by Kurt Rubach, paramedic). I provided a zoomed in view on Thursday to make them a little more obvious.
What I didn’t tell you (besides the fact that there were bullet holes) was that there were no pulses in the arm. The patient was hemodynamically stable, so after evaluation in the ED and insertion of a chest tube, he was taken to angio to evaluate the injury location. Unlike many penetrating injuries where the location is obvious, this was a deep mediastinal hit possibly involving Zone I of the neck (thanks Traumahst). Angio was selected because this was in the days before chest CT.
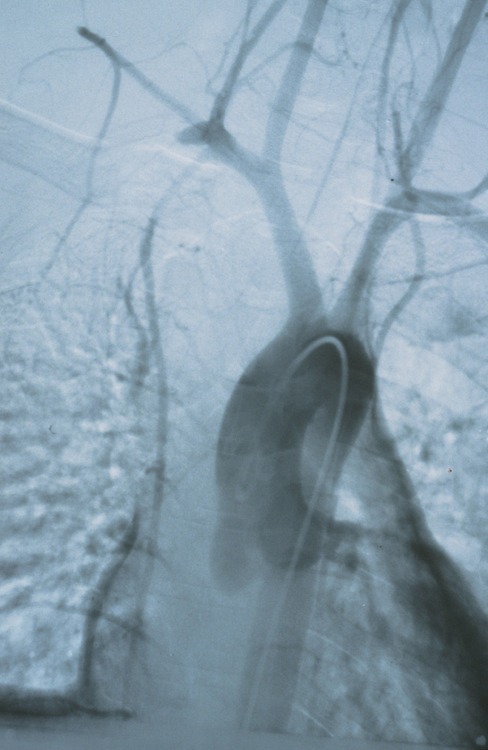
This shows a cutoff of the right subclavian artery. The patient was taken to the OR for sternotomy with a right neck extension and resection of the medial third of the clavicle (see Friday’s xray). The injury was successfully repaired with good return of function, and some residual hemothorax. He was discharged home in a week.
Bottom line: This one was tough because I didn’t give you much of what trauma professionals really need: clinical context. An isolated xray without a clinical history is not enough. It’s very easy to see things that really aren’t there and end up on a wild goose chase. Keep that in mind the next time you expect your radiology colleagues to come up with miracle diagnoses while sitting in a darkened room. Give them the whole story, or have them pop over to the ED to see for themselves.
