To summarize: stab to the back, prone position, stable vitals, awake and alert and breathing easily. The patient had a chest xray which showed some likely hemothorax. He was sent to CT (prone) and the image obtained looked like this:
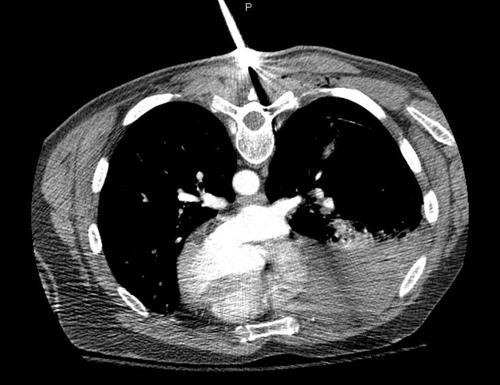
They key points to note are:
- The injury is completely above the diaphragm. No need to worry about an intra-abdominal problem.
- The amount of hemothorax is moderate. It is not enough to mandate a thoracotomy. At least for now.
- There is a significant pneumothorax. You can’t see it due to the windows used, but the lung has separated from the chest wall by about 3cm.
- The track of the knife was directed laterally.
- No significant vascular structures were involved, and there is no contrast extravasation.
Final management: The patient was returned to the ED, and the knife was deftly removed and processed properly as evidence. The patient was then turned supine and a 40 Fr chest tube was inserted using procedural sedation. About 400 cc of blood was drained and reinfused. A repeat chest xray was obtained, which showed some residual hemothorax and near resolution of the pneumothorax. He was then admitted for frequent vital signs and drainage measurements for two shifts. Afterwards, he was placed in our chest tube management protocol. The tube was removed and he was discharged two days later. There were no complications.
