It’s Massive Transfusion Protocol (MTP) week! I’m releasing the next Trauma MedEd newsletter to subscribers at the end of the week, which deals with advanced MTP topics. So leading up to that, I’ll be reviewing the basics for the next several days. I’ll start today with tips on how to build a solid MTP at your center.
Your massive transfusion protocol is a complex set of processes that touch many, many areas within your hospital. There are five basic components (and a few sub-components) to any MTP, so let’s dig into them one by one. They are:
- Universality
- Activation
- Logistics
- Components
- Runners
- Documentation
- Coolers
- Deactivation
- Analysis
Let’s scrutinize each one, starting with the first two today.
Universality. This means that there should be one, and only one MTP in your hospital. I’ve seen some hospitals that have one MTP for trauma, one for cardiothoracic surgery, one for OB, one for GI, and on and on. Yes, each of those services deals with patients who are suffering from blood loss. But it’s the same blood that your trauma patients lose! There’s no need to create a protocol for each, with different ratios, extra drugs, etc. This can and will create confusion in the blood bank which may lead to serious errors.
Activation. This consists of two parts: how do we decide to activate, and then how does everyone involved find out that the MTP is actually being activated? I’ll discuss activation criteria on Thursday. But what about the notification process? Phone call? Order in the electronic medical record (EMR)? Smoke signals?
The most reliable method is a good, old-fashioned phone call. Do not use your EMR except for documentation purposes. Unless there is a very reliable system in the blood bank that translates an EMR order into an annoying alarm or flashing lights, don’t rely on this at all.
Then decide upon the minimum amount of information that the blood bank needs to begin preparing blood products. This usually consists of a name or temporary patient identifier, sex, and location of activation. Ensure that an ID or transfusion band is affixed to the patient so that wrong blood products are not given in multiple patient events.
Tomorrow, I’ll continue with the logistics of the MTP.
And don’t forget to subscribe to TraumaMed if you want to get a full newsletter discussing advanced MTP topics this Friday. Otherwise, you’ll be reading a post on CT scans and rib fractures in the elderly! Subscribe and download back issues by clicking here.
Links: (note – future links will not be live until 9am the day they are published)
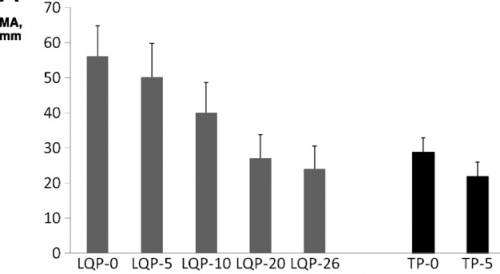 (TEG MA for liquid (LQP) and thawed (TP) plasma
(TEG MA for liquid (LQP) and thawed (TP) plasma