Looks like I failed to give the link to the August TraumaMedEd newsletter. But thanks for all the new subscriptions. I’ve corrected the original post, and here’s the link again!
All posts by The Trauma Pro
Air Travel After Pneumocephalus: Part 2
I’ve previously written about air travel after pneumothorax. The issue is that air expands as you ascend to aircraft level heights. That means that air bubbles in your chest can double or almost triple in size on the average airliner at altitude. For the official recommendations for when it is safe to travel after a pneumothorax, see the link to my previous post below.
And I covered pneumocephalus previously as well. This is a very infrequent condition, and there is very little literature about it. After doing a thorough search, I found two additional papers on it. The first was a computer simulation from Sweden. As expected, it found that air bubbles expand 30% when cabin altitude reaches 8000 ft. They were also able to model changes in intracranial pressure (ICP), and found that it increased as well. The amount was related to the size of the original air bubbles and the rate of the ascent (faster ascent = higher ICP). The worst case ICP increase with a 30cc bubble was 11 torr.
The other paper was from the UK and described a survey of neurosurgeons regarding their advice to patients on air travel after craniotomy. The fear is that there may be residual bubbles around the brain from the surgery. The results of this type of survey are usually all over the place, and more so when you ask neurosurgeons. To their credit, 92% advised their patients not to fly for a period of time. Unfortunately, the timeframes ranged from <2 to >8 weeks!
How about some practical info? I previously wrote about an actual clinical study by the US military who transported soldiers with pneumocephalus by air. Their series of 21 patients showed no neurological deterioration during flight, and 3 who had ICP monitors had no significant changes in pressure.
Bottom line: Computer models (and common sense) tell us that it’s a bad idea to fly commercially with air around your brain. It may work for the military because they have to fly, and the soldier is in a flying ICU. But in civilian aircraft, there is little to be done if medical problems occur short of an emergency landing and transport to a hospital. What’s the magic number of weeks to wait to fly? That is not known, but 2 weeks has worked well for pneumothorax so it seems like a reasonable place to start. But it should be easy for someone to do a retrospective review of serial head CTs from craniotomy patients to see how long it takes for the bubbles to actually reabsorb. And don’t worry about helicopter flights; altitudes are too low to make a difference!
Related post:
References:
- Air transport of patients with intracranial air: computer model of pressure effects. Aviat Space Environ Med Feb 74(2):138-44, 2003.
- Air travel after intracranial surgery: a survey of advice given to patients by consultant neurosurgeons in the UK. Br J Neurosurg 2012 Aug 30, epub ahead of print.
TraumaMedEd Newsletter for August
The newest TraumaMedEd newsletter is out! It was emailed to subscribers on Monday. This months focus is prehospital, with articles on the following:
- Hare traction application
- Trauma care and HIPAA, demystified
- Trauma patient survival and air transport
- What happens when you violate resuscitation guidelines for traumatic cardiac arrest?
- Handoff issues between prehospital and the trauma team
Subscribe to the newsletter by clicking here!
Trauma Residents: How To Remember Liver Anatomy
In trauma surgery, operative management of liver injury is usually messy business, with little time for nice anatomic resections. However, an understanding of the basic anatomy, especially that of the vascular supply is crucial for saving your patient.
A cool tool for remembering Couinaud’s segments and the overall layout of liver anatomy was published in the Archives of Surgery recently. It makes use of a model, which consists of your hand! Just make a fist with your right hand and tuck the thumb behind the other fingers.
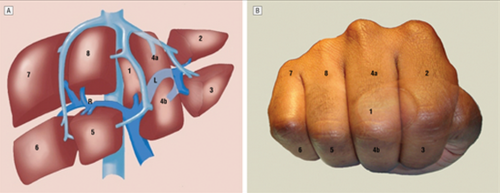
The fingers can then be numbered according to the Couinaud segments, with the caudate lobe (segment 1) represented by the thumb that is tucked away. The PIP joints represent the plane that the portal vein runs through, with branches going to upper and lower segments. Note how the ring finger normally lies a little more anterior than the little finger in this position, just like the sectors of the right lobe.
The creases between the fingers represent the left, middle and right hepatic veins.
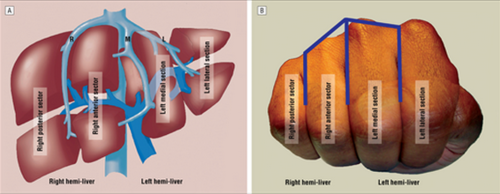
The right hepatic vein is located between the right anterior and posterior sectors and the left hepatic vein sits between the left medial and lateral sectors. The middle hepatic vein is in between the left and right hemi-liver.
Bottom line: This “handy” liver model is available immediately in the OR and is already sterile. It can help visualize liver structures that may be injured quickly and accurately to speed your operative approach to the problem.
Reference: A Handy Tool to Teach Segmental Liver Anatomy to Surgical Trainees. Arch Surg 147(8):692-693, 2012.
PAs and NPs In Level I Trauma Centers
Trauma service staffing is important to maintaining trauma center status. Teaching centers in the US have been grappling with resident work hour rules, and non-teaching centers have always had to deal with how to adequately staff their trauma service. What is the impact of staffing a trauma center with midlevel practitioners (MLPs) such as physician assistants and nurse practitioners?
A state designated Level I trauma center in Pennsylvania retrospectively examined the effect of adding MLPs to an existing complement of residents on their trauma service. They examined the usual outcomes, including complications, lengths of stay, ED dwell times and mortality.
Here are the more interesting results:
- ED dwell time decreased for trauma activations and transfers in, but it increased for trauma consults. Of note, data on dwell times suffered from inconsistent charting.
- ICU length of stay decreased significantly
- Hospital length of stay decreased somewhat but did not achieve significance
- The incidence of most complications stayed the same, but urinary tract infection decreased significantly
- There was no change in mortality
Bottom line: There is a growing body of literature showing the benefits of employing midlevel providers in trauma programs. Whereas residents may have a variable interest in the trauma service based on their career goals, MLPs are professionally dedicated to this task. This study demonstrates a creative and safe solution for managing daily clinical activity on a busy trauma service.
Reference: Utilization of PAs and NPs at a level I trauma center: effects on outcomes. J Amer Acad Physician Assts, July 2011.