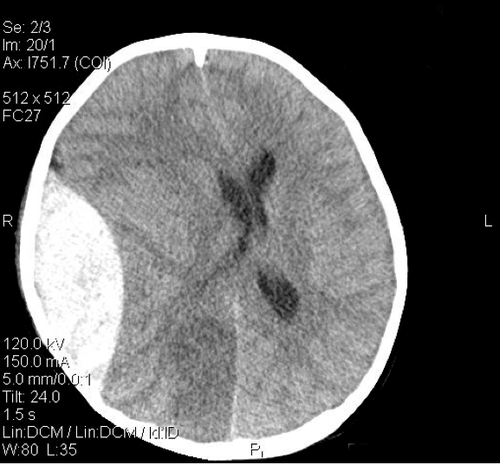
Yesterday, I wrote about an 8 year old bicyclist struck by a car. He had sustained a head injury with a large epidural hematoma and was taken immediately to the OR for evacuation. During the case, the vitals began to suffer. The question was, what would you do as you are called into the room to “fix” this?
There was some excellent chatter on this, and universally, people voted to stick to the ABCs. As taught in ATLS, when the vital signs go awry, the only problems that can cause this degree of sudden derangement start with A, B, C and occasionally D.
The first thing to do is recheck the adequacy of the airway. Sure, the child is intubated. But the neurosurgeon had to position the head, and anesthesia’s access to this area is more limited than in other procedures. Your anesthesiologist is able to put a fiberoptic scope into the mouth and visualize that the tube does indeed pass through the vocal cords. Oxygen saturation is 100% and ETCO2 is 33.
Next, check breathing. The numbers above are helpful, but not the complete answer. Get access to the chest, look and listen. There is good, symmetric chest rise with ventilation, and breath sounds are completely normal bilaterally. The trachea is midline.
Now, is there any circulation problem (bleeding)? There are 5 areas where you can bleed to death:
- Chest – the initial chest xray and your exam make this unlikely.
- Fractures – you examine all extremities and can’t find any gross fractures
- Pelvis – the initial portable xray did not show any fractures, and your exam is normal
- Floor – your shoes are not getting sticky and the OR table is clean (except for the neurosurgeon’s mess)
- Abdomen – ???
Hmm, the abdomen appears a bit distended, and it’s a bit tympanitic. This is a problem area! Let’s say FAST is not available to you, and the pressure is not improving with fluid and pressors.
How can you evaluate this child’s abdomen in this situation? I want the gory details, and will provide answers tomorrow.