The April newsletter is now available! Click the image below or the link at the bottom to download. This month’s topic is “ED Stuff”.
In this issue you’ll find articles on:
Lots of info on trying to use an electronic trauma flow sheet
How do you dress your trauma team?
Subscribers received the newsletter earlier this week. If you want to subscribe to get early delivery in the future (and download back issues), click here.
Over the years I’ve seen a number of trauma professionals, both surgeons and emergency physicians, order liver transaminases (SGOT, SGPT) and bilirubin in patients with liver laceration. I’ve never been clear on why, so I decided to check it out. As it turns out, this is another one of those “old habits die hard” phenomena.
Liver lacerations, by definition, are disruptions of the liver parenchyma. Liver tissue and bile ducts of various size are both injured. Is it reasonable to expect that liver function tests would be elevated? A review of the literature follows the typical pattern. Old studies with very few patients.
From personal hands-on observations, the liver tissue itself tears easily, but the ducts are a lot tougher. It is fairly common to see small, intact ducts bridging small tears in the substance of the liver. However, larger injuries can certainly disrupt major ducts, leading to major problems. But I’ve never seen obstructive problems develop from this injury.
A number of papers (very small, retrospective series) have shown that transaminases can rise with liver laceration. However, they do not rise reliably enough to be a good predictor of either having an injury, or the degree of injury. Similarly, bilirubin can be elevated, but usually not as a direct result of the injury. The most common causes are breakdown of transfused or extravasated blood, or from critical care issues like sepsis, infection, and shock.
Bottom line: Don’t bother to get liver function tests in patients with known or suspected injury. Only a CT scan can help you find and/or grade the injury. And never blame an elevated bilirubin on the injury. Start searching for other causes, because they will end up being much more clinically significant.
References:
Evaluation of liver function tests in screening for intra-abdominal injuries. Ann Emerg Med 20(8):838-841, 1991.
Markers for occult liver injury in cases of physical abuse in children. Pediatrics 89(2):274-278.
Combination of white blood cell count with liver enzymes in the diagnosis of blunt liver laceration. Am J Emerg Med 28(9):1024-1029, 2010.
Patients with traumatic brain injury (TBI) severe enough to cause bleeding are usually admitted to the hospital for observation and in many cases, repeat CT scanning. Those with small intracranial hemorrhages (ICH) may experience progression of the bleeding, and a small percentage of cases may need operative intervention (1-3%). Questions we typically face are, how long should we watch for progression, and how often should we scan?
A retrospective cohort study was carried out at UMD-NJ, looking for answers for a specific subset of these patients. Specifically, they had to have a mild blunt TBI (loss of consciousness and/or retrograde amnesia, GCS in the ED of 13-15) and a positive head CT. They classified any type of hemorrhage into or around the brain as positive.
During a 3 year period, 474 adults were enrolled but only 341 were eligible for the study. They were excluded due to previous injury, presence of a mass (not trauma), need for immediate neurosurgical intervention, or failure to get a second CT scan. The authors found:
7% of patients were taking anticoagulants! This is surprisingly high. Interestingly, 15 were subtherapeutic, 3 were therapeutic and 2 were supratherapeutic.
Subarachnoid hemorrhage was the most common finding on CT (54%). Intraparenchymal hemorrhage was next most common (48%) Many patients had more than one type of bleed.
The injury worsened between the first and second scans in 31% of patients. This number increased to 46% in patients taking anticoagulants.
About 97% of bleeds stopped progressing by 24 hrs post-injury.
Bottom line: Most centers are probably overdoing the observation and repeat scan thing. More than two thirds of bleeds are stable by the first scan (first and second scans identical), and nearly all stop progressing within 24 hours. It’s very likely that patients who are not on anticoagulants and who have a stable neuro exam and stable symptoms can get just one scan and 24 hours of observation. Persistent headache, nausea, failure to ambulate well, or other symptoms warrant a repeat scan and longer observation.
The books all say “transport the patient with an impaling object in place” and “only take the impaling object out in the operating room.” Is this realistic? How do you actually take that knife out?
First, you need to decide if the patient belongs in the OR right now. Are they hemodynamically unstable? Is there obvious arterial bleeding? If so, don’t dawdle. Proceed to the operating room and surgically expose the problem completely.
If the patient is safe to stay in the ED, do what you need to figure out the exact anatomy of the wound (and object). This may involve imaging, usually CT scan. Once the exact position of the object is understood, build an anatomical picture of the situation in your mind. What named arteries might be involved? What other vital structures?
Given this anatomic information, a decision can then be made regarding the best location for removal. The majority of the time, this will be in the operating room. It is best to obtain optimum surgical exposure prior to pulling it out. In the abdomen, this is easy. However, some areas (skull, sinuses) are tricky and may not require exposure of the end of the tract. Visualization of the remaining hole(s) is key so that bothersome bleeding can be recognized immediately.
The object should be grasped firmly and carefully and removed in one smooth motion. Visual monitoring for five minutes will virtually eliminate the presence of bleeding. If it does occur, then deeper exploration is warranted. In the awake patient, I generally push gently on either side of the entry point prior to and during the pull to provide some sensory distraction. Then I hold pressure on the site for 5 minutes (no peeking) to assure myself that there is no bleeding.
And don’t forget the forensics! Let the police photograph the patient. Handle the object carefully so as not to disturb any fingerprints. Place it carefully in a paper bag, labelled appropriately. And always make sure that a chain of evidence form is properly filled out so it and the object itself can be handed over to the proper authorities.
There’s a lot of confusion about subdural pathology after head trauma. All subdural collections are located under the dura, on the surface of the brain. In some way they involve or can involve the bridging veins, which are somewhat fragile and get more so with age.
Head trauma causes a subdural hematoma by tearing some of these bridging veins. Notice how thick the dura is and how delicate the bridging veins are in the image below.
When these veins tear, bleeding ensues which layers out over the surface of the brain in that area. If the bleeding does not stop, pressure builds and begins compressing and shifting the brain. A subdural hematoma is considered acute from time of injury until about 3 days later. During this time, it appears more dense than brain tissue.
After about 3-7 days, the clot begins to liquefy and becomes less dense on CT. Many hematomas are reabsorbed, but occasionally there is repeated bleeding from the bridging veins, or the hematoma draws fluid into itself due to the concentration gradient. It can enlarge and begin to cause new symptoms. During this period it is considered subacute.
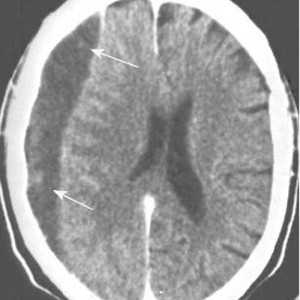
It moves on to a more chronic stage over the ensuing weeks. The blood cells in it break down completely, and the fluid that is left is generally less dense than the brain underneath it. The image below shows a chronic subdural (arrows).
Hygromas are different, in that they are a collection of CSF and not blood. They are caused by a tear in the meninges and allow CSF to accumulate in the subdural space. This can be caused by head trauma as well, and is generally very slow to form. They can lead to slow neurologic deterioration, and are often found on head CT in patients with a history of falls, sometimes in the distant past. CT appearance is similar to a chronic subdural, but the density is the same as CSF, so it should have the same appearance as the fluid in the ventricle on CT.