There is a fairly robust amount of data that shows that, properly performed, the cervical spine can be cleared using a high quality CT read by a highly skilled radiologist. This is true even for obtunded patients. Pooled data suggest that the miss rate in this group is only 0.017%. And MRI is not perfect either, missing significant ligamentous injury in a small number of patients.
But it seems that some trauma professionals are still using MRI in some cases despite this data. The latest study on MRI focuses on the cost-effectiveness of the technique. The authors selected patients with GCS < 13 to be their obtunded group, which is probably a bit high. Nevertheless, they used a fairly sophisticated (meaning hard to understand) modeling-based decision analysis using a computerized simulation. This allowed them to compare different clearance strategies without performing large randomized clinical trials.
The authors considered MRI vs no MRI, false results, collar use and complications, MRI use with cost and complications, and the worst-case scenario of tetraplegia. Here is a flow chart of the scenarios considered. (Courtesy JAMA Surgery)
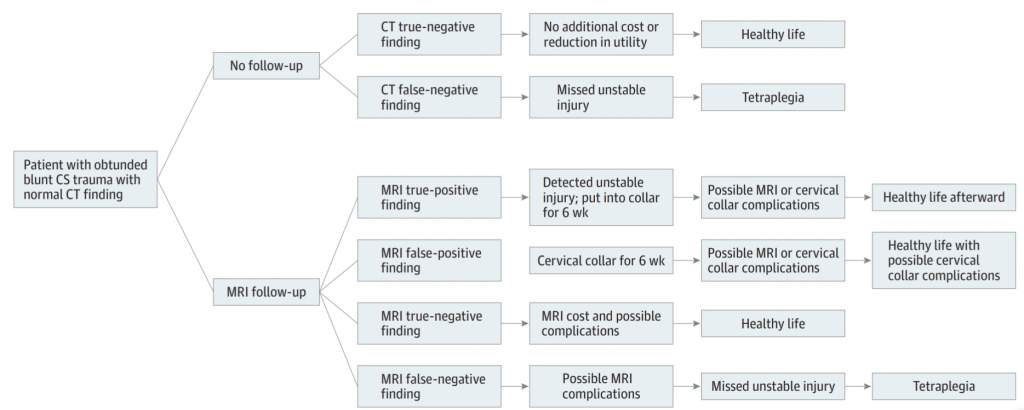
Here are the factoids:
- The mean cost for followup vs no followup was $14K vs $1K, with no increase in quality adjusted life years (QALY)
- No followup was the better strategy when the negative predictive value of CT was high (>98%), when the risk of an unstable injury treated with a collar turning into a permanent deficit was >25%, or if the chance of a missed injury becoming a permanent deficit was >58%
- No followup MRI was the better strategy in all 10,000 iterations of the simulation
Bottom line: Yes, this is a fairly heavy computer simulation. But the reality is that we will never be able to design a large enough study to critically evaluate this issue and have it pass any IRB review. So it’s probably as good as it will ever get. It’s time to stop wasting money and putting obtunded patients in harm’s way by locking them into a relatively inaccessible MRI scanner for 30 minutes just to confirm the CT. Or keeping a collar until until the skin breaks down.
Here is a copy of the practice guideline we use for clearing all cervical spines, obtunded or not. Yes, there is some weirdness with soft collars, which mainly serve as a reminder to re-examine the patient at some point. But note the scan technique and requirement that it be read by a neuroradiologist for final clearance.
Related link:
Reference: Cost-effectiveness of Magnetic Resonance Imaging in Cervical
Clearance of Obtunded Blunt Trauma After a Normal
Computed Tomographic Finding