Despite all you read about it these days, REBOA is still very new. The first papers describing use in humans are barely 5 years old! A few select centers have been early adopters and are publishing a regular flow of research on their experience.
But we need more numbers! Many trauma centers have considered, or actually adopted the use of REBOA already. However, we are still working out a lot of the nuts and bolts of this very invasive procedure. The group at University of Arizona – Tucson reviewed the national experience over a two year period by massaging the data in the Trauma Quality Improvement Program (TQIP) database. All Level I-III trauma centers in the US are required to report their experience to this large, detailed collection of trauma data.
They performed a retrospective review of REBOA vs non-REBOA patients matched for demographics, prehospital and emergency department vital signs, mechanism of injury, degree of pelvic disruption in pelvic fracture patients, solid organ injuries, and lower extremity fractures and vascular injuries. The studied outcomes were complications and mortality.
Here are the factoids:
- Nearly 600,000 records were scanned for the two year period, and only 140 REBOA patients were identified (!)
- These 140 REBOA patients were matched with 280 similar non-REBOA patients
- Average age was 44 and average ISS was 29, 74% were males and 92% were blunt trauma
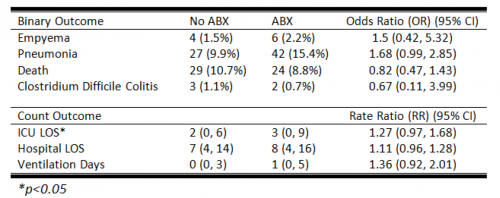
- Overall complication rate was 7.4% and mortality was 25%
- There was no difference in 4-hour or 24-hour numbers of blood, plasma, or platelets transfused
- ICU and hospital length of stay were identical
- 24-hour mortality in the REBOA group was significantly higher (36% vs 19%)
- REBOA patients were significantly more likely to require amputation (5% vs 1%)
Bottom line: These are not great numbers for REBOA! What gives? There are a number of possibilities:
- It’s a database study, so some key information might be missing
- The numbers remain small, only 140 patients out of half a million records in two years!
- There is no way to know how the patients were selected for REBOA
- The experience and skill level at the hospital performing the procedure is not known
- The interplay of other injuries and comorbidities is unclear
- And many more…
BUT, the numbers are concerning. The early adopter centers have better outcomes, and this has prompted many centers with fewer eligible patients to jump on the bandwagon. We all need to remember that this is a brand new procedure and we are still learning the nuances. It is extremely important that every center performing REBOA contribute their results to a national registry. We still need to figure out which patients will benefit from it, how it should be used, and how we can minimize complications and maximize survival in our patients.
Reference: Nationwide analysis of resuscitative endovascular balloon occlusion of the aorta (REBOA) in civilian trauma. Session I Paper 5, AAST 2018.