Any trauma performance improvement professional understands the importance of undertriage and overtriage. Overtriage occurs when a patient who does not meet trauma activation criteria gets one anyway. And undertriage is the converse, where no activation is called despite criteria being met. As you may expect, the latter is much more dangerous for the patient than the former.
I frequently get questions on the “Cribari grid” or “Cribari method” for calculating these numbers. Dr. Chris Cribari is a previous chair of the Verification Review Subcommittee of the ACS Committee on Trauma. He developed a table-format grid that provides a simplified method for calculating these numbers.
But remember, the gold standard for calculating over- and undertriage is examining each admission to see if they met any of your trauma activation triage criteria. The Cribari method is designed for those programs that do not check these on every admission. It is a surrogate that allows you to identify patients with higher ISS that might have benefited from a trauma activation.
So if you use the Cribari method, use it as a first pass to identify potential undertriage. Then, examine the chart of every patient in the undertriage list to see if they meet any of your activation criteria. If not, they were probably not undertriaged. However, you must then look at their injuries and overall condition to see if they might have been better cared for by your trauma team. If so, perhaps you need to add a new activation criterion. And then count that patient as undertriage, of course.
I’ve simplified the calculation process even more and provided a Microsoft Word document that automates the task for you. Just download the file, fill in four values in the table, update the formulas and voila, you’ve got your numbers! Instructions for manual calculations are also included. Download it by clicking the image below or the link at the end of this post.
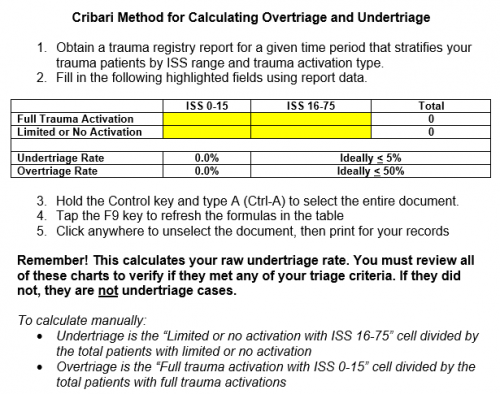
Download the calculator by clicking here
In my next post, I’ll examine how the NFTI score (need for trauma intervention) fits into the undertriage/overtriage calculations.
Related posts: