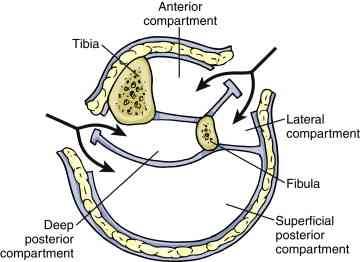
It seems like this topic keeps on coming up! This is the second article I’ve seen this year that describes a variation on the single-incision leg fasciotomy. In the classic two-incision approach, the lateral incision gives access to the anterior and lateral compartments, and the medial incision to the posterior and deep posterior. See below.
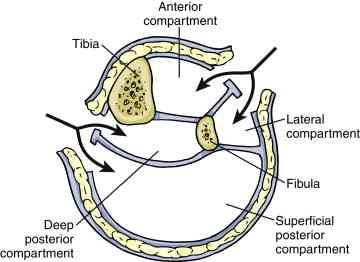
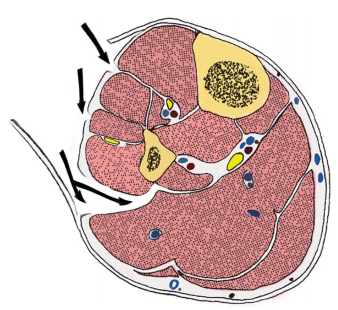
The more “standard” single-incision approaches either go through (i.e. removes part of) or around, the fibula. In the diagram below, the arrows point to the access points into the anterior, lateral, posterior and deep posterior from top to bottom.
In the “new” variation described, the authors slide along the lateral edge of the tibia to get to the deep posterior compartment.
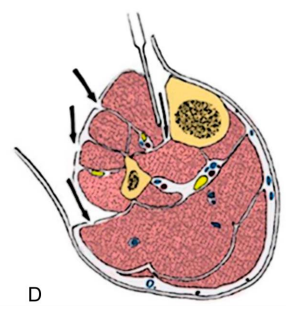
This approach requires stripping the tibialis
anterior muscle away from the tibia, which some orthopods may argue interferes with healing. And, as with the other single-incision technique, the procedure may take additional time.
Bottom line: I’m still not a big fan of single-incision fasciotomy. My main reason is that most surgeons are not as familiar with the technique. And patients who have a potentially limb threatening process are not the best to learn on. I have seen too many incomplete fasciotomies with persistent compartment syndrome in my career.
So unless you are being mentored by someone who is well versed in the technique, use the two incision technique and use a cadaver to practice your single incision operation.
Reference: A Single-Incision Fasciotomy for Compartment Syndrome
of the Lower Leg. J Ortho Surg 30(7):e252-e255, 2016.