In my last post, we looked at our knowledge base regarding the use of unfractionated heparin versus low molecular weight heparin. And the latter won. Today, let’s dig into the question of early versus late prophylaxis in patients with TBI and intracranial hemorrhage.
Neurosurgeons are remarkably cautious when considering anticoagulant thromboprophylaxis in these patients. Obviously, there is always concern for making the bleeding worse. This is very undesirable where there is little extra space and drainage is complicated.
But as we know, dogma about these issues tends to get spread very easily, with little scientific support. Let’s review another systematic review and meta-analysis (see last post) that examines the question.
As is usual, there have been a lot of contributions to this area over the years. Unfortunately, many are not entirely related to the question or have significant bias or design flaws. Of a total of 1,490 papers identified by the authores during PubMed searches only 29 were on topic. And of these only 11 were suitable for analysis. Early prophylaxis was defined as within 72 hours, although the authors were able to slice and dice this into shorter intervals.
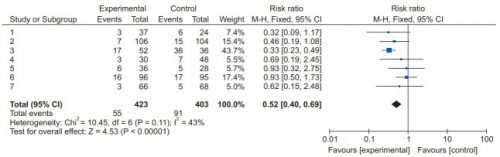
Here are the results:
- Progression of hemorrhage. There was no significant progression of intracranial bleeds seen at 24, 48 or 72 hours. However, this result is probably somewhat biased by the fact that fewer patients with severe injury are enrolled in studies of VTE prophylaxis. The overall odds ratio for early vs late administration was 0.86 favoring early prophylaxis. However, the confidence interval crossed the midline, so there was no difference noted in progression of bleed or mortality with early VTE prophylaxis.
- Occurrence of DVT. Many of the studies indicated a decrease in VTE in the patients given early prophylaxis. This was noted at all three time intervals as well. The overall odds ratio was 0.58, which was statistically significant. This means that patients with early prophylaxis at any point had their risk of VTE reduced almost by half.
- All cause mortality. Could their be other issues with early VTE prophylaxis that would increase mortality? This analysis showed that the odds ratio was 0.83 favoring early prophylaxis decreasing it. This is a 17% reduction in mortality, but unfortunately was not statistically significant. Although there is a trend toward lower mortality with early prophylaxis, it is not significant.
Bottom line: Again, this type of analysis is powerful but can suffer from the combined weaknesses of its individual papers. However, the best information we have thus far shows that early prophylaxis prior to 72 hours of admission does not appear to be harmful, does not result in progression of intracranial bleeding or excess mortality, and cuts the risk of VTE almost in half.
In my next post, I’ll explore a recent paper that examines how early we can really go with VTE prophylaxis.
Reference: Clinical outcomes following early versus late pharmacologic thromboprophylaxis in patients with traumatic intracranial hemorrhage: a systematic review and meta-analysis. Neurological review 43:861-872, 2020.