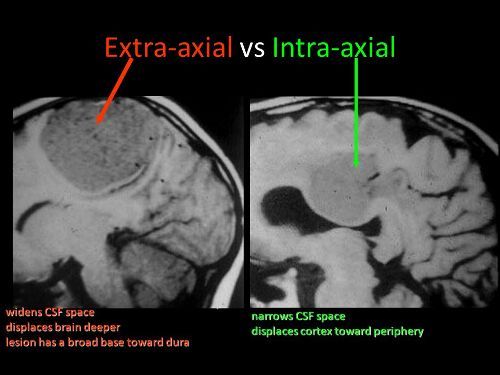
You’ve seen it on head CT reports. “The patient has a collection of extra-axial blood…” Then it goes on to describe the location and size of a subdural hematoma. But why is it called “extra-axial?”
The answer lies in the embryology of the central nervous system. Yes, it’s been a long time since any of us have read anything about that. Early animals had a straight neural tube, which slowly evolved into a brain and spinal cord. This is known as the axis of the nervous system.
The brains of early vertebrates developed at the end of the neural tube, and were oriented in the same longitudinal axis as the rest of it. As brains got bigger, a 90 degree bend occurred at the cephalic flexure.
So in humans, there is a difference between the body axis and the brain axis. But the brain axis is what really counts. This means that any blood outside of the brain axis is defined as extra-axial.
Bottom line: Extra-axial blood is defined as any bleeding outside of the brain parenchyma. This includes subdural and epidural hematomas, and subarachnoid hemorrhage. It does not include any intraparenchymal bleeding like contusions, strokes, or hematomas.
Blunt injury to the carotids or vertebrals (BCVI) is a little more common than originally thought, affecting about 1% of blunt trauma patients. We have many tools available to help us diagnose the problem: duplex ultrasound, CT angiography (CTA), MR angiography (MRA), and even good old conventional 4 vessel angiography.
But which one is “best?” This is a tough question, because there is always some interplay between clinical accuracy and cost. The surgical group at the Medical College of Wisconsin – Milwaukee did a nice job teasing some answers from existing literature on the topic. The authors tried to take a comprehensive look at costs, including money spent to prevent stroke, the cost of complications of therapy, and the overall cost to society if the patient suffers a stroke.
Here are the factoids:
For patients at risk for BCVI, the stroke rate is 11% without screening, 6% with duplex ultrasound screening, 4% with MRA, and 1% with either CTA or conventional angiography
From a societal standpoint (includes the lifetime costs of stroke for the patient), CTA is the most cost effective at $3,727 per patient
From the hospital standpoint (does not include lifetime cost), no screening is the most cost effective, but has the highest stroke rate (11%)
CTA prevents the most strokes, and costs about $10,000 per patient while decreasing societal costs by about $32,000 per patient screened
Bottom line: The “best” test for patients at risk for blunt cerebrovascular injury is the CT angiogram. It minimzes the stroke rate, and provides information on all four vessels supplying the brain, which is probably why the duplex ultrasound has a higher miss rate (can’t see the vertebrals or into the skull). But how do you decide who is at risk for this problem. Tune in tomorrow!
Reference: Screening for Blunt Cerebrovascular Injuries is Cost-Effective. J Trauma 70(5):1051-1057, 2011.
With the implementation of resident work hour restrictions 10 years ago, resident participation in clinical care has declined. In order to make up for this loss of clinical manpower and expertise, many hospitals have added advanced clinical providers (ACPs, nurse practitioners and physician assistants). These ACPs are being given more and more advanced responsibilities, in all clinical settings. This includes performing invasive procedures on critically ill patients.
A recent study from Carolinas Medical Center in Charlotte NC compared complication rates for invasive procedures performed by ACPs vs residents in a Level I trauma center setting.
A one year retrospective study was carried out. Here are the factoids:
Residents were either surgery or emergency medicine PGY2s
ACPs and residents underwent an orientation and animal- or simulation-based training in procedures
All procedures were supervised by an attending physician
Arterial lines, central venous lines, chest tubes, percutaneous endoscopic gastrostomy, tracheostomy, and broncho-alveolar lavage performances were studied
Residents performed 1020 procedures and had 21 complications (2%)
ACPs performed 555 procedures and had 11 complications (2%)
ICU and hospital length of stay, and mortality rates were no different between the groups
Bottom line: Resident and ACP performance of invasive procedures is comparable. As residents become less available for these procedures, ACPs can (and will) be hired to take their place. Although this is great news for hospitals that need manpower to assist their surgeons and emergency physicians, it should be another wakeup call for training programs and educators to show that resident education will continue to degrade.
Reference: Comparison of procedural complications between resident physicians and advanced clinical providers. J Trauma 77(1):143-147, 2014.
Yesterday, my colleague the Skeptical Scalpel wrote about an interesting (?) paper published in Emergency Medicine Australasia. It was a small study that concluded that ED wait times decreased as the number of people presenting to be seen decreased. Where’s the mystery in that? Overstating the obvious?
But if you look through almost any journal today, you will find studies that leave you wondering how they ever got published. And this is not a new phenomenon. Look at any journal a year ago. Five years ago. Twenty years ago. And even older. The research landscape is littered with their carcasses.
And on a related note, sit down with any serious clinical question in your field you want to answer. Do a deep dive with one of the major search engines and try to get an answer. Or better yet, let the professionals from the Cochrane Library or other organization do it for you. Invariably, you will find hints and pieces of the answer you seek. But never the completely usable solution you desire.
Why is it so hard? With tens of thousands of articles being published every year?
Because there is no plan! Individuals are forced to produce research as a condition of their employment. Or to assure career advancement. Or to get into medical school, or a “good” residency. And in the US, Level I trauma centers are required to publish at least 20 papers every three years to maintain their status. So there is tremendous pressure across all disciplines to publish something.
Unfortunately, that something is usually work that is easily conceived and quickly executed. A registry review, or some other type of retrospective study. They are easy to get approval for, take little time to complete and analyze, and have the potential to get published quickly.
But what this “publish or perish” mentality promotes is a random jumble of answers that we didn’t really need. There is no planning. There is no consideration of what questions we really need to answer. Just a random bunch of easy to get published thoughts that never get cited by anyone else.
Bottom line: How do we fix this? Not easily. Instead of focusing on the quantity of publications, the “authorities” need to focus in on their quality. Extra credit should be given to multicenter trial involvement, prospective studies, and other higher quality projects. The actual number of publications should not matter as much as how much high quality work is in progress. Sure, the sheer number of studies published will decline, but the quality will increase exponentially!
EAST just published their newest practice management guideline, which pertains to rectal trauma. They sought to answer three questions that pertain to nondestructive penetrating trauma to the extraperitoneal rectum.
Trauma dogma from the 80′s and 90′s mandated that these injuries undergo three things: proximal diversion, distal rectal washout, and presacral drainage. The latter two have had waning interest over the intervening years, and questions have even been raised as to whether diversion is really necessary.
Practice Guideline Committee members at EAST performed a thorough and well documented review of the existing literature to determine what we really should be doing with these injuries.
Here are the factoids:
Proximal diversion. The major fear that prompts surgeons to divert is the possibility of infectious complications in the area of the rectal injury itself, or death. The literature consisted of 14 papers, most of which were retrospective and observational. Although there was no difference in mortality (about 0%), the incidence of infections doubled in patients without diversion. The recommendation was that patients with these injuries receive a proximal diverting colostomy.
Presacral drains. Only 17 papers addressed this question, and they were of low quality with few patients. There is not enough evidence to recommend this practice. And from a logistical standpoint, I could never figure out why this should work. The drain is placed in the presacral space, adjacent to the posterior rectum. How can this do anything for an anterior injury?
Distal rectal washout. In the good old days, this was performed through the distal portion of the newly created colostomy. There were all kinds of fancy ways to do it, and it required converting to lithotomy position and stationing someone (hint: intern) with a bag or bucket to catch the effluent. Very messy and unpleasant. Only 13 papers addressed this practice, and could not convincingly demonstrate a benefit. Not recommended.
Some additional tips of my own:
Do not violate the peritoneal reflection in the pelvis while doing the laparotomy. If the injury is isolated to the distal rectum, you will create a conduit for infection in the deep pelvis. You will have a hard time repairing an injury from above, especially in the usual narrow male pelvis. Don’t look at it; just let it heal on its own.
Create a standard end colostomy. Surgeons argue that a loop colostomy is convenient because it may be possible to close it later without reopening the midline incision. This is not always the case, and the bridge that is necessary to keep the loop above the skin makes colostomy care very difficult. Patients frequently complain about smelly leaks.
Bottom line: EAST guidelines are helpful in figuring out what to do in certain clinical situations, but they do not provide detailed guidance. This guideline provided answers (as best they could) to just three questions about rectal trauma. They justify not doing things that most surgeons have not been doing for some time. But don’t try to talk yourself out of not doing the diverting colostomy.
Reference:
Management of penetrating extraperitoneal rectal injuries: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma 80(3):546-551, 2016.
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.