So our patient has presented to your ED, on foot, with a steak knife sticking out of his head! You’ve activated your trauma team, so now what do you do?
As always, start with a thorough physical exam. A good exam of the head is imperative, as is a scrupulous neurologic exam. In this case, the blade enters just below the right eye, traveling front to back and staying just about level.
Make sure there are no other injuries. Remember the Dang Factor! Don’t focus on the knife and miss other important injuries. And by all means, don’t take it out in the ED!
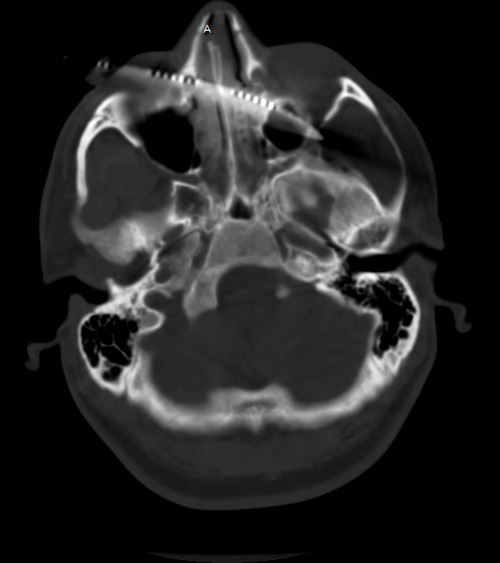
Since this patient is stable and neurologically intact, the surgeons will want a better idea of the structures involved under the skin. CT is the best tool for this, although there will be scatter from the metal. Here is a representative image:
So now, think about how you will get this out. Tweet and comment your answers.
Related post: