The use of medical helicopters has grown at an astonishing rate in the 10+ years since Medicare got involved with payment for this service. All high level trauma centers have helicopter landing facilities, and many either own or are a part owner in at least one helicopter EMS service (HEMS).
Here’s a state by state breakdown of the number of medical helicopters:
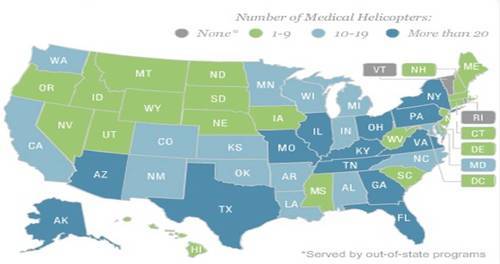
It’s gotten to the point where the indication for summoning a HEMS service seems to be the presence of a patient to ride on it!
A lot of papers have been published in the past 20 years trying to justify the benefits of using these services. As is the usually case when a lot of papers are published on one subject, most of them are not very good. Lots of studies have been performed to try to justify their use, and most were not successful. The following items have been scrutinized:
- Interfacility transfers
- Trauma
- Pediatric transfers
- Pediatric trauma
- Burns
- OB
- Neonatal
- Rural trauma
Most of these papers found little, if any, benefit. The ones that did tended to be published by institutions that owned these services, raising the question of bias. The one thing that was always significantly different was the cost. HEMS costs at least 10 times more that ground EMS transport.
So the benefits are not very clear. What about the risks? I’ll talk about those tomorrow.
Related posts: